

The Big Short: Covid
The Big Short: Covid
How an Outsider on Twitter is Beating Public Health at its own Game

Michael Lewis wrote the wrong book.
The Premonition, published in May 2021, profiles a group of American scientists and public health officials ringing alarm bells about pandemic preparedness leading up to covid and in its early days. Lewis portrays this collection of mavericks as our saviours from covid, if only the lethargic US government and the disobedient American public would heed their calls for aggressive public health action. The cast of characters includes Carter Mecher, long-time advocate for school closures in a pandemic and Charity Dean, former Assistant Director of the California Department of Public Health. “The greatest trick the CDC ever pulled was convincing the world containment wasn’t possible,” Dean says in The Premonition.
Lewis, at least at the time the book was published, was captivated by the narrative of the aggressive scientist and public health officer as underdog, fighting against the institutional bias to inaction. “There are times when working on this it reminded me a bit of The Big Short,” said Lewis in a 60 Minutes interview. Really? The Big Short, perhaps Lewis’ most well-known work, profiles a group of outsiders that successfully predict and profit from the US housing collapse in 2008. They have no business possessing unique insight relative to those on the inside at large banks and asset managers and yet, through careful analysis and quirks of personality, they execute enormously profitable trades.
The book that Michael Lewis should have written, The Big Short: Covid, goes like this. Governments, public health, and media have gone one way globally on pandemic response – significant and broad-based intervention. Lockdowns, masking, vaccine passports, travel restrictions. The wave of consensus opinion on these issues is so overwhelming that to question it invites labels of misinformation and conspiracy. Yet against the tsunami of public pressure, there is a group of outsider Ontarians coming to different conclusions about the correct path forward. Like Michael Burry reading through thousand-page mortgage-backed security prospectuses, this group is scavenging government databases to carefully tease out insights about the pandemic, and to police the policies and pronouncements of our leaders. Active on Twitter and often anonymous, this group has no business coming to insightful conclusions. But somehow, they are.
The right book for Mr. Lewis to write about covid would be about one of these outsider Ontarians – Kelly Brown.
It began innocently enough. It was early in the pandemic, March 2020. Countries around the world scrambled to lock down amid frightening headlines. The stock market tanked and Kelly Brown needed to know what all of this meant for his investment portfolio. So he did what he does best: he crunched some numbers. It was a matter of life and death as well as dollars and cents.
A former Bay Street analyst, Kelly spent the better part of the last decade managing his own and his family’s capital. He was no stranger to intensive research. His due diligence on a company could last months, scrounging around for every piece of data and information available. He applied the same discipline to his early work on covid. Almost immediately Kelly recognized that the alarming estimates of a 2-3% death rate were too high1. The real figure appeared to be closer to 1%, still as much as ten times higher than the seasonal flu, but even the 1% figure was likely an overestimate. While the numerator, the number of deaths was relatively knowable, the denominator, the total number of infections, was underestimated because not all people infected with covid test positive (there are asymptomatic cases, some people will choose not to be tested).
Even more important than the average death rate was the stratification of disease by age and health status. “Just like a company where a headline revenue or earnings number may conceal different trends among business lines or a hidden asset, the overall death rate for covid masked varying risks by age and health status,” Kelly says. Covid could be very dangerous to the elderly and sick but thankfully almost completely spared the young and healthy.
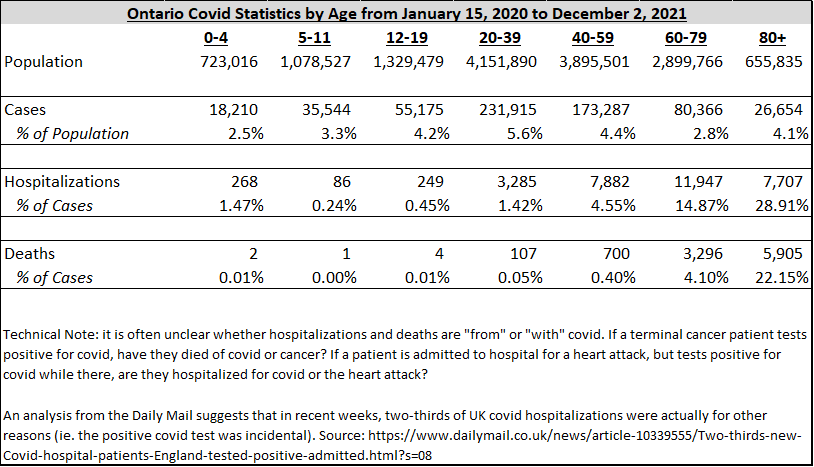
According to data from Ontario on pandemic-to-date cases, hospitalizations and deaths, those over age 80 have a risk of death that is more than 3,000 times higher than those under the age of 20. Those between the ages of 60 and 79 are 90 times more likely to experience a fatal outcome from covid than those in their twenties and thirties. The Public Health Agency of Canada has also disclosed that 90% of covid-19 deaths in Canada from March to July 2020 occurred in individuals with pre-existing chronic conditions2 (the same figure for the US, as per the CDC is 95% and on average those dying of covid have four co-morbidities3). According to Statistics Canada, the average age of those that died of covid in 2020 was 84 years old4. With these insights in-hand, Kelly concluded that the broad-based lockdowns were an overreaction. “I’m not saying we should have done nothing, just that the response needs to be proportional to the threat,” he reflects. Kelly aggressively bought the decline in the stock market.
Through the summer of 2020, with life returning to normal, Kelly focused on his investment portfolio while paying peripheral attention to media coverage of the pandemic. He was surprised that media, politicians, and public health officials weren’t more focused on the age stratified risk profile. Young healthy people, especially kids, were not at risk from the virus. This was fantastic news, there was no reason to be fearful. And yet, it almost seemed at times like those in charge of pandemic response actually wanted to promote fear.
In April 2021, reports emerged in The Telegraph that SAGE, an advisory body guiding the UK government’s response to the pandemic, had recommended in a March 2020 report that “the perceived level of personal threat needs to be increased among those who are complacent, using hard-hitting emotional messaging,” and that, “a substantial number of people still do not feel sufficiently personally threatened; it could be that they are reassured by the low death rate in their demographic group [emphasis mine].”5 SAGE was not alone in its push for fear. Former Trump advisor Scott Atlas relayed this anecdote from a 2020 discussion with Anthony Fauci in his book A Plague Upon Our House:
“’So you think people aren’t frightened enough?’
[Fauci] said, ‘Yes, they need to be more afraid.’”
Still, in spite of the fear, Kelly believed that reason would prevail. A whole-of-society shutdown simply would not make sense in future waves in light of the stratified risk profile. Kelly saw merit to the approach advocated by professors from Harvard, Stanford and Oxford in the Great Barrington Declaration: “The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk. We call this Focused Protection.”6
Schools are a safe setting because the risk to students from covid is minimal, below that of the seasonal flu, while less than 10% of teachers are above age 60. The harms from school closures are significant, so they should remain open. In contrast, major effort should be taken to ensure long-term care facilities are protected with frequent testing and PPE as well as quarantine protocols for residents that contract the virus. Focused protection was the best strategy to balance safety with disruption to society.
In late Summer, with cases ticking higher, Kelly was disappointed when the Ontario government tightened restrictions. On September 8th, further reopening was “paused” by Minister of Health Christine Elliott. Then, on September 17th, Premier Doug Ford reduced the number of people permitted at private gatherings. Fearing another dark Winter with all-of-society restrictions, Kelly took to Twitter to share his insights. “I thought I had something to say and that I had a professional Twitter following that would respect the quality of the work,” he says. “There was a feeling of shouting into the abyss. Where else do I say this?” He christened himself “Accidental & unofficial COVID-19 data analyst” on the social media site.
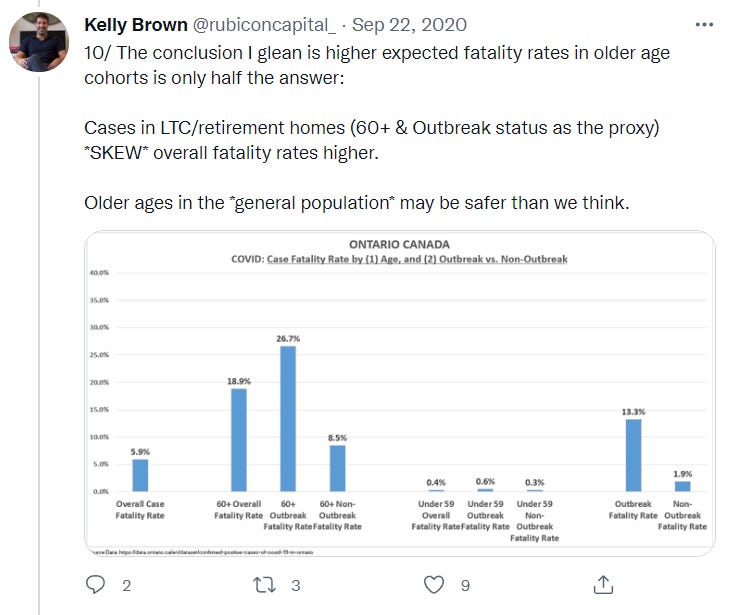
Kelly’s first tweets about covid, published September 22nd, were short on flair but heavy on substance. “Cases in LTC/retirement homes…skew overall fatality rates higher,” he tweeted. “Older ages in the general population may be safer than we think.” In other words, the age stratification analysis needed further stratification. Those over 60 living in a retirement home or long-term care setting had a fatality rate that was more than three times that of people over 60 not living in an institutional setting. The risk from covid was concentrated in long-term care facilities. No need for across-the-board lockdowns, just do focused protection.
Kelly’s concern grew as restrictions in Ontario were tightened over the Fall, culminating in Doug Ford’s December 21, 2020 announcement of a provincewide shutdown. “I had a sense that the lockdowns would not be good for the community or the economy and I was compelled to make sure this was the right approach,” he says. “There was no course correction.”
In the early days of the pandemic, with a lot of uncertainty about the virus and its impact on the healthcare system, a temporary shutdown seemed logical. This is an unprecedented situation that could be disastrous – let’s take a brief pause to orient our response. But with the data now in and the risk highly, highly stratified, blanket lockdown policies inflicted meaningful harm on populations that were not at risk from the virus while providing questionable benefits in terms of reduced transmission and illness7. For example, closing university campuses removes students from a very low-risk setting and distributes them back throughout society where they can potentially infect others at high risk of a severe outcome from the virus. It seemed our leaders committed to a course of action and were unwilling to deviate as the facts changed.
This experience – call it commitment or confirmation bias or simply an unwillingness to change your mind – is familiar to all investors. After taking a position in a stock, the mind plays tricks on itself to distort reality, to preserve the investor’s ego and avoid admitting a mistake. Unfortunately, it was also familiar to Kelly, just having taken a painful (and public) loss in 2019.
Kelly was raised in Chatham, a small city in Southwestern Ontario. Growing up, he would often make the short drive to his family’s greenhouse farm in nearby Leamington. He loved walking the houses and still visits the farm regularly, now in the hands of his uncle and cousin. So when Kelly stumbled upon Bevo Farms, a specialized greenhouse operator out of Vancouver run by a father-son team, he was favourably inclined. Bevo’s business was greenhouse propagation, an intricate and operationally challenging part of the greenhouse growing cycle. Bevo would raise the crop for the early part of its life and then sell it on to another farm to grow to maturity. In Kelly’s view, management’s long track record in this tricky business meant they must be strong operators. He started buying shares around the $1.50 range in 2017.
In the Fall of 2018, Bevo merged with a company in the sizzling cannabis sector, becoming Zenabis. Canada recently legalized marijuana, igniting a rush to construct greenhouse space to meet demand from the nascent legalized market. The stock rocketed higher, tripling from $2 up to $6. Kelly had faith in the father-son team managing the business, Jack and Leo Benne. Given their background in the technically challenging propagation business, “I thought they would be the best weed growers,” Kelly says.
As the stock retraced some of its move higher, falling back to $3 per share, Kelly went public on Twitter, arguing the shares were undervalued relative to other companies in the industry. The stock seemed to be ignored by other investors, there were no Bay Steet analysts publishing research on Zenabis. With years of experience and training in finance, Kelly trusted his instincts.
The response on Twitter was, well, not what Kelly was hoping for. Skepticism about Zenabis was high and many criticized the report. Detractors argued that the company was late to the game, competitors had already built out a lot of greenhouse capacity and there was only so much demand. Zenabis risked bringing new acreage to market late at a time when there was already too much supply. “The Twitter feedback was really the first piece of disconfirming evidence,” says Kelly, “but I dismissed the concerns.”
Kelly thought he was the expert on the stock. Having performed in-depth due diligence and meeting with management, all supported by years of investment experience, he discounted the contrary opinions. That he recently made his views public on Twitter didn’t help – to completely reverse his decision so quickly would have felt like a public admission of failure. And so Kelly downplayed another piece of disconfirming information in late March. Zenabis executed a large financing on expensive terms from a low-quality lender. “If the company was really so great, why couldn’t they get attention from a better lender?” Kelly asks himself rhetorically, with the full benefit of hindsight. The stock drifted below $3.
Over the Winter, Kelly used Twitter to highlight the inappropriateness of the blunt all-of-society lockdowns and to counteract the fear broadcast by the media and public health officials. On December 27, 2020, just as the winter lockdown commenced in Ontario, Kelly argued on Twitter that a province-wide shutdown was illogical when some regions were barely impacted by covid: “North and East Ontario. 15 of 34 Public Health Units. ~3.06m people. 57 COVID19 hospitalizations. Locked down.”

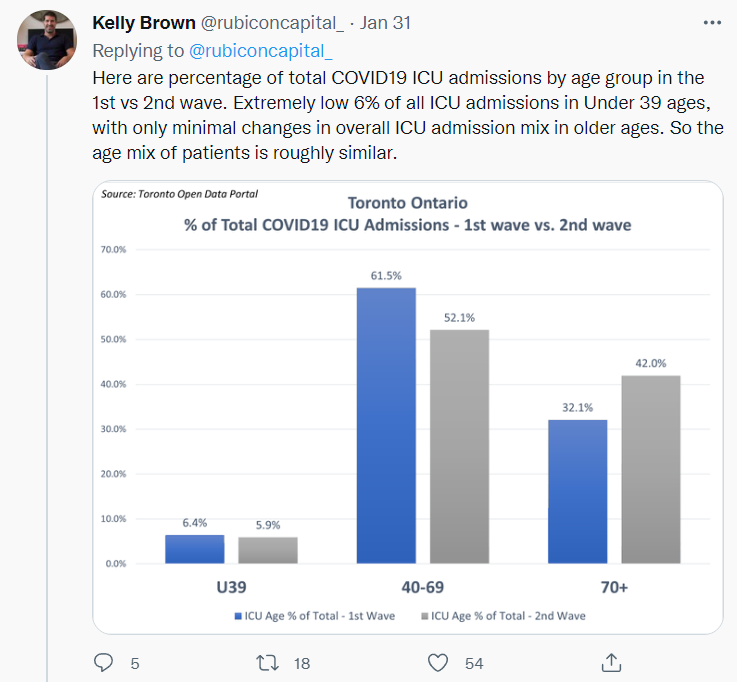
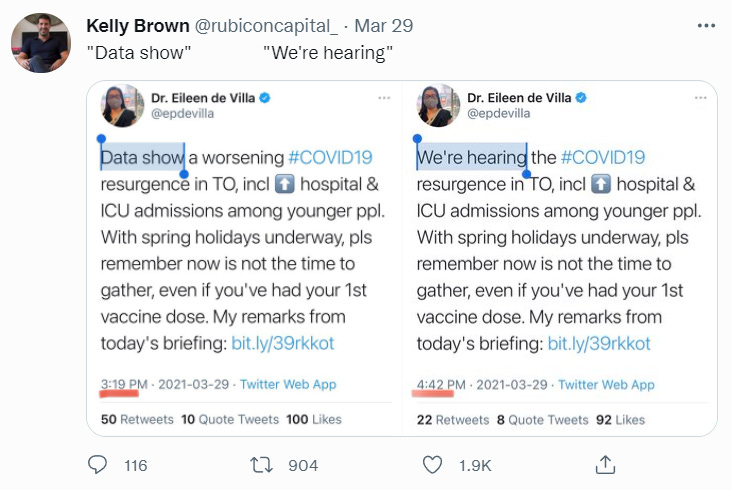
Kelly also followed up a Toronto Star article about growing ICU admissions among younger patients during the second wave with some hard facts. Turns out only 6% of ICU admissions were under 39 years old and, in contrast to claims in the article, the rate was effectively unchanged from the first wave to the second. Plus, he began poking fun at some of our public health officials, including Dr. Eileen de Villa, Medical Officer of Health for the City of Toronto. In a March tweet sent at 3:19 pm, de Villa wrote, “Data show [emphasis mine] a worsening #COVID19 resurgence in TO, incl [higher] hospital & ICU admissions among younger ppl…”. Less than two hours later, at 4:42 pm, the tweet was revised to, “We’re hearing [emphasis mine] the #COVID19 resurgence in TO, incl [higher] hospital & ICU admissions among younger ppl…”.

By mid-2021, Kelly’s following on Twitter had blossomed to over 10,000 accounts. With the blunt lockdown policies and the media’s emphasis on fear over data, Kelly’s “antenna was up” about everything to do with covid. When assessing a management team that had revealed themselves to be dishonest, Kelly would “read every filing”, carefully parsing each comment management made, never giving the benefit of the doubt. The vaccines had now become the focus of the covid response, safe and effective we were promised. As with the lockdown policies earlier in the pandemic, Kelly set about verifying this claim through data.
Ontario collects reports of negative vaccine reactions in the Adverse Events Following Immunization (AEFI) database. The reports range from a sore arm and fever up to heart attack and death. There are two challenges when using the database to assess vaccine safety – did the adverse events actually occur and, even if the event happened, was it caused by the vaccine or did it just coincidentally occur following vaccination. For the former issue, AEFIs in Ontario are reported by health care providers or vaccine recipients and all AEFIs are investigated, assessed and documented by public health units. AEFIs are categorized as “serious” or “non-serious”. According to the province, “due to data limitations and the relatively brief follow-up period of AEFIs reported in Ontario, AEFI reports that meet the serious definition typically have an in-patient hospitalization or death reported [emphasis mine]8.”
So, for serious AEFIs at least, we can be confident that something has gone wrong with the patient because they have typically presented to hospital. Whether the vaccine caused the issue or is merely associated with it is still an open question. A certain number of people are going to have a heart attack this month, whether they receive a vaccine or not. So if everyone receives a vaccine today, some people will have a heart attack after receiving a vaccine. This doesn’t mean the vaccine caused the heart attack. However, if the population-wide rate of heart attack increases after the vaccines, or if a certain group that typically does not experience heart trouble finds themselves in cardiac arrest, perhaps something is going wrong. Enter myocarditis.
On August 25th, Public Health Ontario published a special report on myocarditis and pericarditis following covid-19 vaccination9. Kelly highlighted the findings of this report in a September 3rd tweet, “WE ARE HARMING YOUNG MEN…@PublicHealthON reports 1 in 3,800 risk of myo/pericarditis in 18-24 males after 2nd Moderna dose.” Myocarditis and pericarditis are inflammation of the heart muscle or the tissue surrounding the heart muscle. Of the cases included in the special report, 98% included a visit to the emergency room and two-thirds were hospitalized. The risk of a serious outcome from covid in this age group is low.
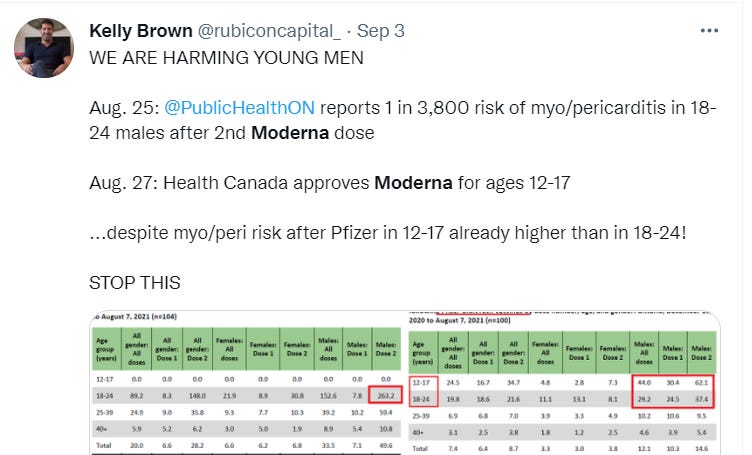
Myocarditis is rare among young and healthy people and the increase in myocarditis incidents coincided with the vaccine roll-out. This didn’t appear to be a statistical fluke, and the province was conceding as much with the publication of its special report. Kelly also noticed that the population-level myocarditis rates concealed important differences by age, gender, and vaccine manufacturer. The average risk of myocarditis across all ages and genders for a two-dose course of the Pfizer vaccine was about 1-in-46,000 as of early September. But the risk for 18-24 year old males of two doses of the Moderna vaccine was 1-in-3,350 (vs. roughly 1-in-14,000 for Pfizer at the time). Why was Moderna causing more myocarditis than Pfizer? The quantity of MRNA in the Moderna vaccine is more than three times Pfizer (100 µg vs. 30 µg). Worryingly, the incidence of myocarditis across all ages and both manufacturers was also higher after the second dose, sometimes meaningfully, perhaps suggesting that cumulative heart damage was occurring with each dose.
There is no objective test for the threshold at which a vaccine becomes unsafe. Ontario stopped administering the AstraZeneca covid vaccine with blood clots occurring in about 1-in-50,000 doses administered10. The US CDC recently recommended Pfizer and Moderna be used over Johnson & Johnson’s covid vaccine due to clotting risk of about 1-in-250,000 people11. The clots caused by AstraZeneca and J&J can sometimes be fatal. In 1976, the US halted administration of a swine flu vaccine, in part because of a 1-in-100,000 occurrence of Guillan-Barré syndrome12.
On September 29th, more than a month after publication of the special health report on myocarditis and weeks after Kelly’s tweet, Ontario’s Chief Medical Officer of Health, Dr. Kieran Moore belatedly advised that “out of an abundance of caution” 18-24 year olds should be vaccinated with Pfizer instead of Moderna13. What took so long? Why was Kelly Brown, using the province’s own data, weeks ahead of Ontario’s top doctor? Then, over a month later, on December 3rd, Canada’s Federal National Advisory Committee on Immunization (NACI) updated its recommendation that Pfizer be used on a preferential basis over Moderna for individuals 12-29 years of age in light of the risk of myocarditis14. Again, what took so long?
The NACI report in their recommendation for Pfizer over Moderna notes a rate of myocarditis of 1-in-6,300 second Moderna doses for males 18-29 across Canada. The most recent Ontario data shows a myocarditis rate of 1-in-7,100 for Pfizer second doses in males age 12-1715, within 10% of the rate at which Moderna was eschewed in favour of Pfizer. Recognizing that the threshold for safety is somewhat arbitrary, and that the decision was lower-stakes in the case of Moderna with an alternative available, couldn’t we argue that Pfizer is also unsafe for teenage males at this point?
The press release accompanying Kieran Moore’s September 29th announcement stated: “vaccination is the best way to protect against COVID-19 related complications, and the risk of contracting myocarditis and other serious adverse events including pericarditis, arrhythmia, deep-vein thrombosis, pulmonary embolism, myocardial infarction, intracranial hemorrhage and thrombocytopenia is 18 times higher among patients with COVID-19.” So even though we’re acknowledging that the vaccine is not as safe as we thought, it is still much better to be vaccinated than to get covid. While that may very well be true for most people, this is thesis creep. We went from the vaccines are safe to the harms from covid are worse than the harms from the vaccine.
Adverse events following covid vaccination were not limited to myocarditis. In a tweet from mid-September, Kelly noted that reported serious adverse events following covid vaccination were six and a half times the rate reported for all vaccines from 2012-2019. Could it simply be the case that patients and health care providers are more sensitive to the controversy surrounding the covid vaccines, and so more likely to file a report? Sure. Could it also be that the covid vaccines are actually more harmful than previous vaccines? Yes.

Kelly held on to his position in Zenabis through September when they disclosed that production problems at their facility would delay sales. “Stocks fluctuate. I was anchored to higher prices. I did not want to crystallize the loss,” Kelly says. The stock declined to less than $1. Conviction wavering, Kelly began trimming his position. But he would not sell all his shares until the announcement of a rights offering in October at a dilutive price. “I woke up and realized this was a permanent loss of capital, that the idea of getting my money back was over,” Kelly says. The dilution from the rights offering would be meaningful, the value of the company was permanently impaired. Kelly exited the position in early 2020.
Fortunately for Kelly, the stock market serves up new opportunities every day. The loss on Zenabis was not fatal to his portfolio and by 2021, riding the broader stock market recovery, his investments had reached new all-time highs. Even the best investors aren’t right all the time. In fact, they often make mistakes. Some investors find success even if they are right only half the time by riding winners and cutting losers.
Investors have a highly visible scoreboard with which to assess their performance – stock prices. While the market can be irrational for periods of time, if an investor’s portfolio is not performing, eventually they must conclude that they should not be managing money. But what is the scoreboard for public health? How do we know whether the interventions – lockdowns, masking, travel restrictions, vaccine passports – were the right decisions? There is no one metric like a stock price for public health, the distillation of all policy in one number. Covid cases, hospitalizations, and deaths are too myopic, too singularly focused. Public health is obviously about more than just one virus. Plus, interventions can have an impact on areas like the economy and national morale.
Human beings don’t like to admit when they are wrong. Our minds play all sorts of tricks on us to convince us that we haven’t, in fact, made a mistake. Kelly was understandably reluctant to admit that his Zenabis investment was an error. But that is the beauty of the stock market. There is a natural, unavoidable mechanism of accountability. Like a slap to the face, poor fundamental performance and a falling stock price obligated Kelly to confront reality.
Who or what can force public health to confront the reality of their failing response to the covid pandemic? At what point do we admit to ourselves that the interventions have been too broad and destructive in light of the massive risk stratification profile of the disease? The world is complex. No person, no matter how educated or experienced, has perfect foresight or the ability to anticipate all unintended consequences. We should not be indifferent to new information; we must evolve as necessary.
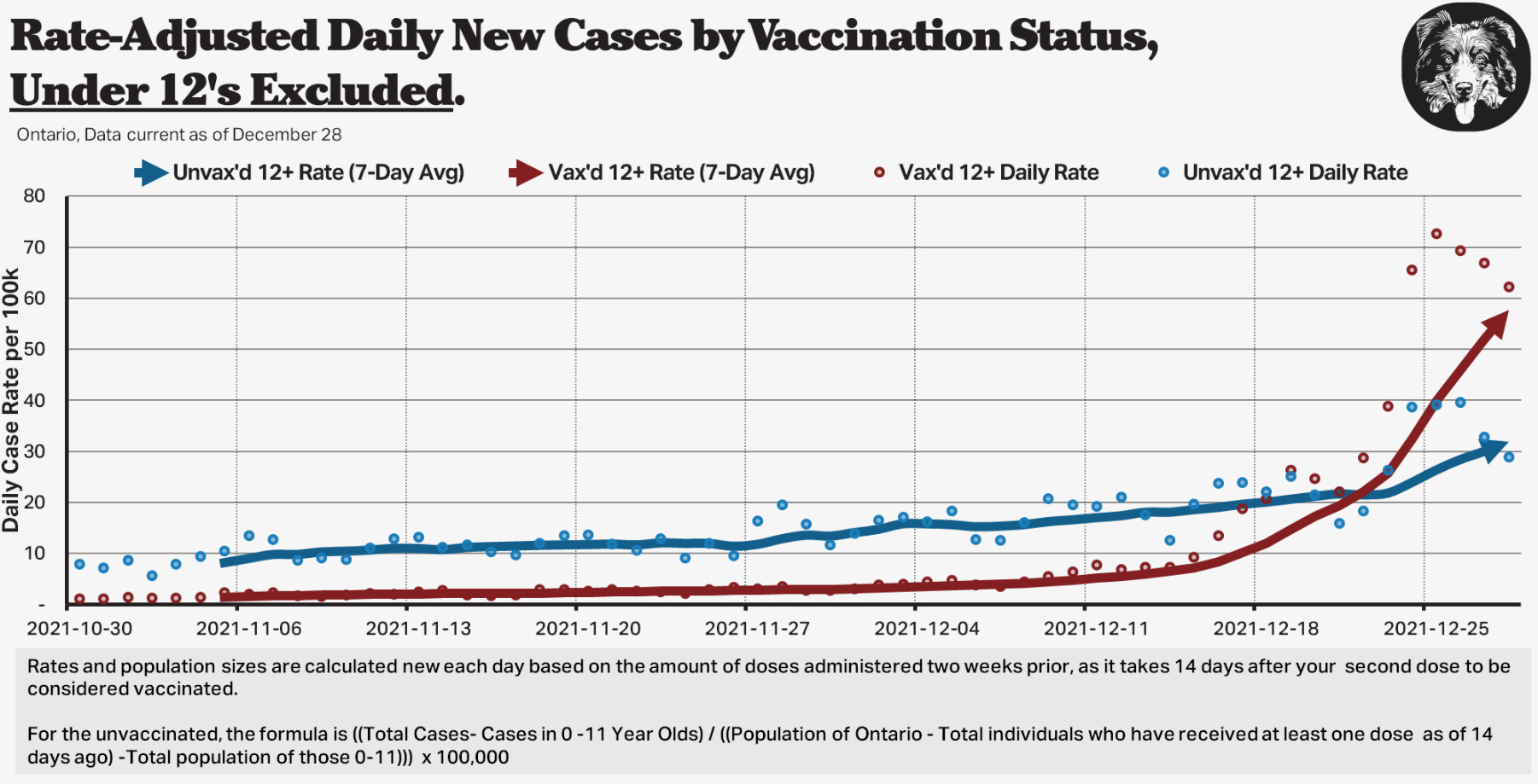
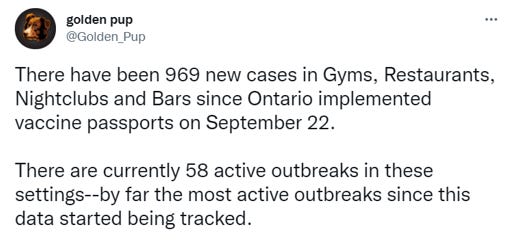
The latest twist is the Omicron variant. Highly contagious, but seemingly less severe16. Due to the number of mutations on the spike protein, the vaccines have lost efficacy against infection, though the manufacturers believe they are still able to prevent severe disease17. Another Twitter outsider - @Golden_Pup – prepares a daily summary of covid cases in Ontario by vaccination status. His analysis shows that case rates among the vaccinated 12 years and up are now roughly double those of the unvaccinated – vaccinated people over 12 are more likely to test positive. Those under 12 are excluded from this analysis because vaccines only recently became available to that group. As recently as early November unvaccinated people were three times more likely to test positive per capita. Pup also keeps a running tally of cases and outbreaks in settings that require a vaccine passport – gyms, restaurants, nightclubs and bars. As of December 20th, there have been 969 cases recorded in settings requiring a vaccine passport since their introduction on September 22nd.
While the moral weight of a vaccine passport and vaccine mandates for employment was always extremely substantial, the real-time data were at least supporting the notion that unvaccinated people were more likely to be infected with and so spread the virus. But that is no longer true, at least to any significant degree. Again, the facts have changed. Where is the course correction from public health? What possible rationale could there be for maintaining these incredibly divisive policies in light of the latest data?
Recently, Kelly’s public message has expanded beyond the numbers to include notes of hope and unity. After two years of fear and division, this is sorely needed. “We are in a battle for hearts and minds,” he says. “We don’t have to live like this. We need to move on from the daily feeling of hopelessness and start to fear the right thing: continued disconnection and depression.”
The public discourse around covid can be divisive and rude, yet somehow Kelly manages to elevate his tone above the fray, staying balanced and fact-based. Perhaps it’s his focus on the data that keeps him grounded. I like to think it’s his perspective, rooted in a long-term historical context. He is a history buff, especially ancient Rome. He named his business Rubicon Capital. “The public health response needs to be proportional to the threat and it needs to course correct in response to new information,” he stresses.
“For vaccinated people, do you not remember that you have your freedoms today because you took a medicine? Freedoms are by right and God-given, not a privilege that can be revoked,” Kelly says. With the roll-out of the third booster and talk of additional shots at least annually going forward, this is not a one-and-done situation. The Government of Canada has ordered enough vaccines from Pfizer and Moderna through 2024 to vaccinate the entire population with at least two doses annually18.
Most Ontarians were vaccinated willingly. Many will wish to take every booster that is offered. But stop for a moment to contemplate the society we have constructed. Should you wish, for whatever reason, not to take an annual or semi-annual booster, you will be forfeiting your right to participate in society. It will become more difficult to work, you will be widely condemned in the media and by those around you, you will be unable to leave the country, or eat in a restaurant, or work out at the gym. In this society, we are all imprisoned; we just purchase our freedom through vaccination, six or twelve months at a time.
https://slate.com/technology/2020/03/coronavirus-mortality-rate-lower-than-we-think.html
https://www.canada.ca/en/public-health/services/diseases/coronavirus-disease-covid-19/epidemiological-economic-research-data/excess-mortality-impacts-age-comorbidity.html
https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html
https://www.canada.ca/en/public-health/services/reports-publications/canada-communicable-disease-report-ccdr/monthly-issue/2020-46/issue-10-october-1-2020/epidemiology-deceased-cases-covid-19.html
https://www.telegraph.co.uk/news/2021/04/02/state-fear-ministers-used-covert-tactics-keep-scared-public/
https://gbdeclaration.org/
For example: https://www.frontiersin.org/articles/10.3389/fpubh.2020.604339/full
“Stringency of the measures settled to fight pandemia, including lockdown, did not appear to be linked with death rate”
https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3665588
“Comparing weekly mortality in 24 European countries, the findings in this paper suggest that more severe lockdown policies have not been associated with lower mortality. In other words, the lockdowns have not worked as intended.”
https://pubmed.ncbi.nlm.nih.gov/33400268/
“[We] do not find significant benefits on case growth of more restrictive non-pharmaceutical interventions (ie. lockdowns).”
https://www.publichealthontario.ca/-/media/documents/ncov/epi/covid-19-aefi-report.pdf?la=en
https://www.publichealthontario.ca/-/media/documents/ncov/epi/covid-19-myocarditis-pericarditis-vaccines-epi.pdf?sc_lang=en
https://www.cbc.ca/news/canada/toronto/ontario-update-astrazeneca-vaccine-1.6022545
https://www.wsj.com/articles/cdc-advisers-review-blood-clotting-risk-associated-with-j-js-covid-19-vaccine-11639662363
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4599698/
https://news.ontario.ca/en/statement/1000907/ontario-recommends-the-use-of-pfizer-biontech-covid-19-vaccine-for-individuals-aged-18-24-years-old
https://www.canada.ca/content/dam/phac-aspc/documents/services/immunization/national-advisory-committee-on-immunization-naci/rapid-response-recommendation-use-covid-19-vaccines-individuals-aged-12-years-older-myocarditis-pericarditis-reported-following-mrna-vaccines/rapid-response-recommendation-use-covid-19-vaccines-individuals-aged-12-years-older-myocarditis-pericarditis-reported-following-mrna-vaccines.pdf
https://www.publichealthontario.ca/-/media/documents/ncov/epi/covid-19-aefi-report.pdf?la=en
https://www.msn.com/en-us/money/other/omicron-infects-70-times-faster-but-is-less-severe-study-says/ar-AARPZEa
https://www.wsj.com/articles/first-big-omicron-study-finds-two-doses-of-pfizers-vaccine-cuts-hospitalization-risk-by-70-11639495432
https://www.canada.ca/en/public-services-procurement/services/procuring-vaccines-covid19.html
Great article that should be a book (then adapted into a movie).